1. Introduction
Resuscitative thoracotomy (RT), also known as emergency department thoracotomy, is a time-critical, high-acuity intervention performed in traumatic arrest or peri-arrest states. It is not a salvage procedure for unsurvivable injury. It is a targeted, physiologically rational intervention designed to correct immediately reversible causes of traumatic circulatory collapse.
In HALO terms, Resuscitative thoracotomy is:
- High Acuity – failure leads to death
- Low Occurrence – infrequently performed
- Time Critical – delays worsen outcomes
- Skill Dependent – requires speed and precision
RT exists within the HALO philosophy: rare, decisive, unforgiving. When indicated, delay equals death. When misapplied, it consumes resources and exposes teams to risk without benefit.
Survival varies widely (approximately 4–33%), heavily dependent on mechanism of injury, time since loss of vital signs, and presence of signs of life prior to arrest
Contemporary series report overall survival around 7–8%, with significantly better outcomes in penetrating thoracic trauma.
2. Physiological Goals of Resuscitative Thoracotomy
The procedure aims to:
- Relieve cardiac tamponade
- Control cardiac and/or pulmonary hemorrhage
- Enable open cardiac massage
- Permit internal defibrillation
- Occlude or cross-clamp the descending thoracic aorta
- Prevent or control broncho-venous air embolism
- Temporize until definitive surgical repair
These objectives must be clear before the scalpel touches skin.
3. Indications
Accepted Indications
Resuscitative thoracotomy is indicated in:
- Penetrating thoracic trauma with cardiac arrest and prior signs of life
- Suspected pericardial tamponade with arrest
- Witnessed traumatic arrest with organized ECG activity
- Blunt trauma arrest with prior signs of life (highly selective)
- Exsanguinating thoracic hemorrhage
- Arrest from extra-thoracic hemorrhage where aortic occlusion may be beneficial
Time thresholds (general guidance):
- Penetrating trauma: <10–15 minutes since loss of vital signs
- Blunt trauma: <5 minutes since loss of vital signs
These are guidelines, not absolutes. Clinical judgment applies, particularly in young patients with limited comorbidity.
4. Contraindications
Resuscitative thoracotomy should not be performed when:
- No signs of life on arrival
- Asystole without tamponade
- Prolonged pulselessness beyond accepted time limits
- Massive, clearly unsurvivable injuries
- Severe non-survivable head injury
- Multiple devastating blunt injuries
Futility must be recognized early. HALO discipline includes knowing when not to cut.
5. Preparation and Prerequisites
Before thoracotomy:
- Secure airway (ETT)
- Bilateral finger thoracostomies
- Large-bore vascular access
- Initiate balanced transfusion
- Limit crystalloid
- Ensure full PPE (double glove, eye protection)
Thoracotomy must not delay reversible arrest interventions.
6. Equipment
Minimum requirements include:
- # 20 scalpel
- Mayo scissors / heavy trauma shears
- Finochietto rib spreaders X2
- Hemostatic clamps and forceps
- Suction
- Non-absorbable sutures (e.g., 3-0)
- Foley catheter (for balloon tamponade of ventricular wounds)
- Internal defibrillator paddles if available
- 30F chest tube
Definitive surgical support must be available. RT is a bridge, not an endpoint.
7. Relevant Anatomy
Key structures:
- Heart and pericardium
- Descending thoracic aorta (left posterior mediastinum)
- Left phrenic nerve (runs longitudinally along pericardium)
- Pulmonary hilum
- Internal mammary vessels
- Esophagus (distinguish from aorta)
Injury to the phrenic nerve or coronary arteries represents preventable error.
8. Technique: Left Anterolateral Thoracotomy
1. Position
- Supine
- Left arm abducted if feasible
- Prep from sternum to posterior axillary line
2. Incision
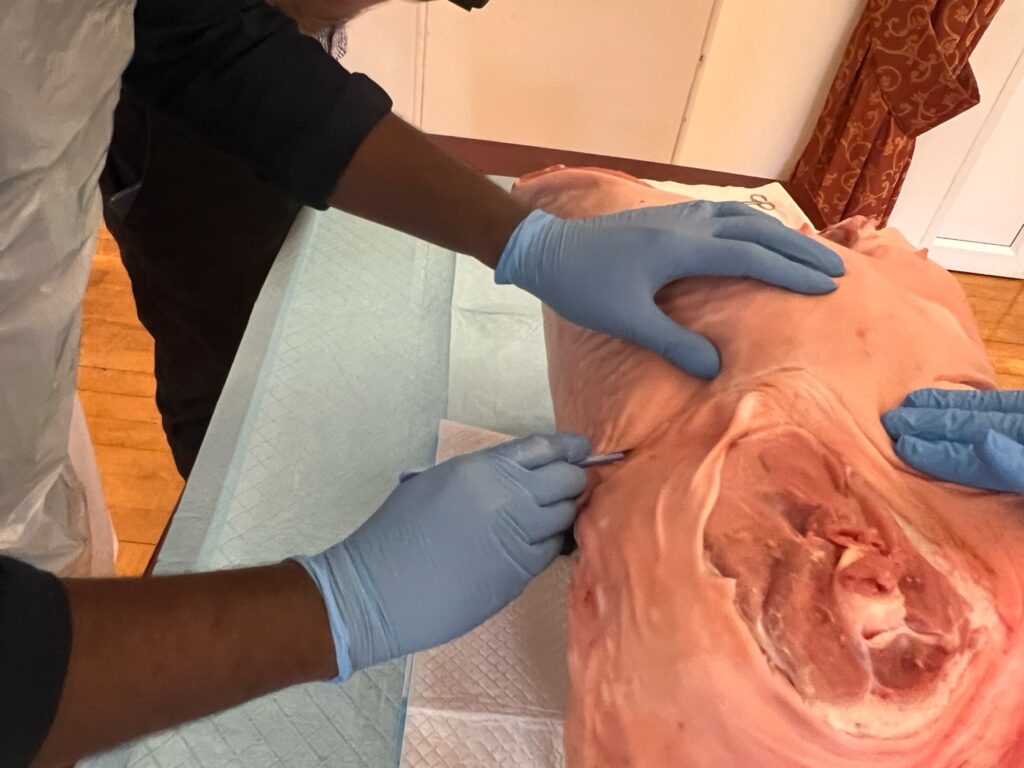
- Fifth intercostal space
- From sternum to mid-axillary line
- Curvilinear, following rib contour
- Incise above rib to avoid neurovascular bundle
3. Enter Chest

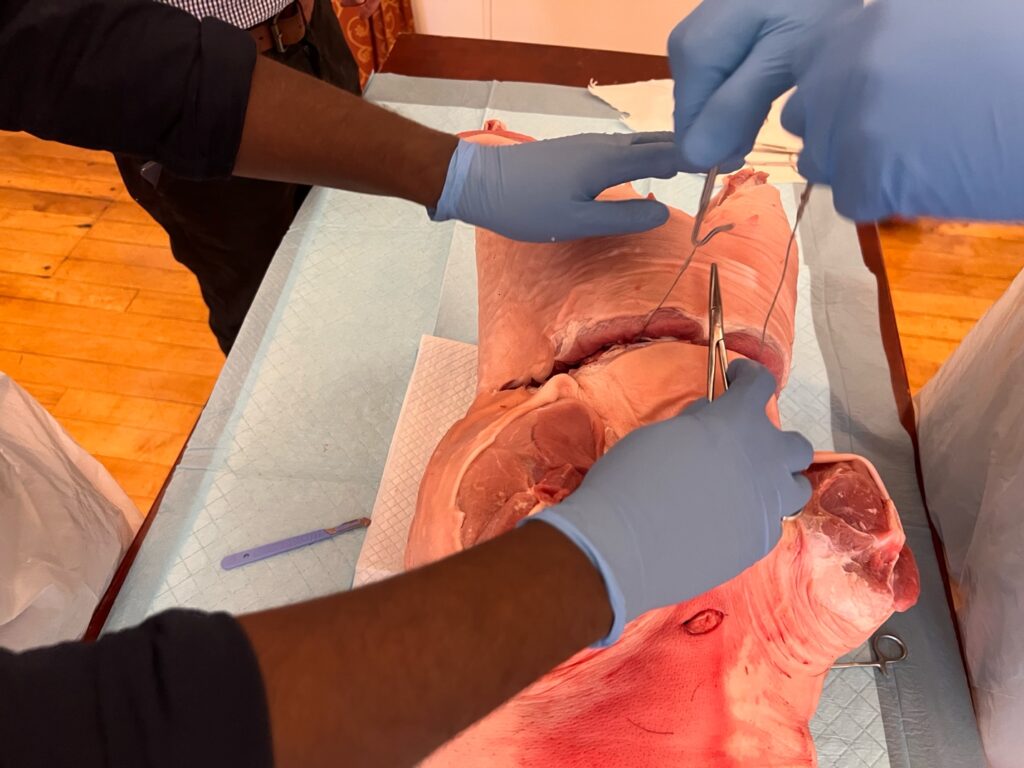
- Use heavy scissors to enter pleura
- Extend incision fully. Similar incision across the other side, meet both incisions in the middle over the sternum
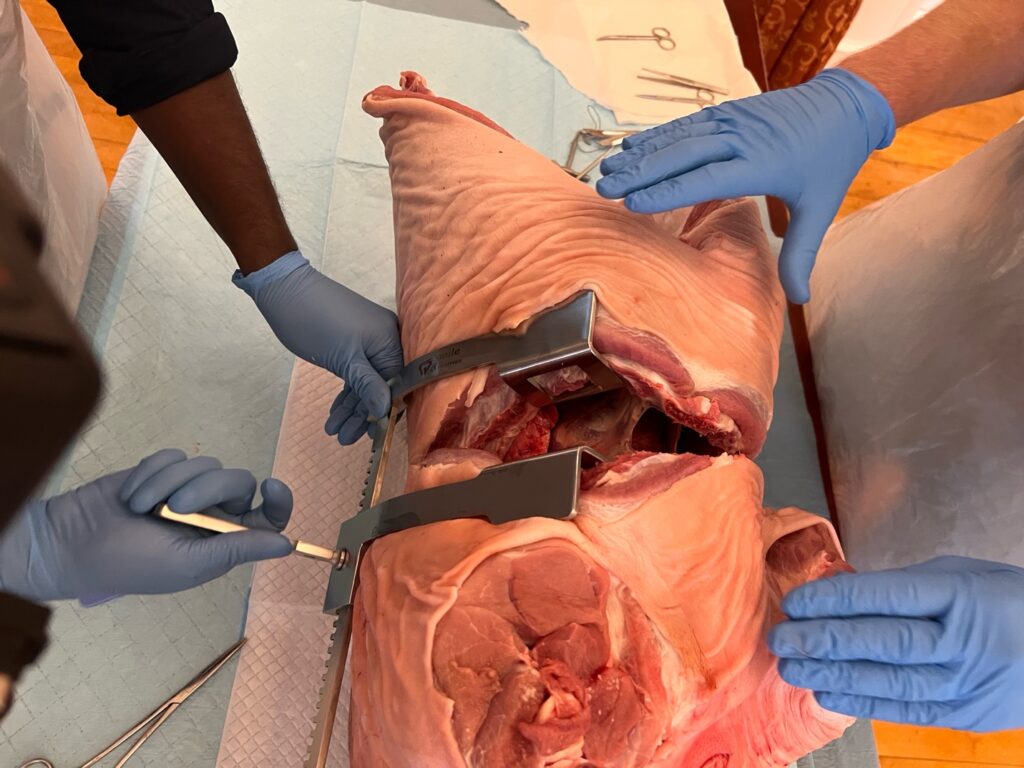
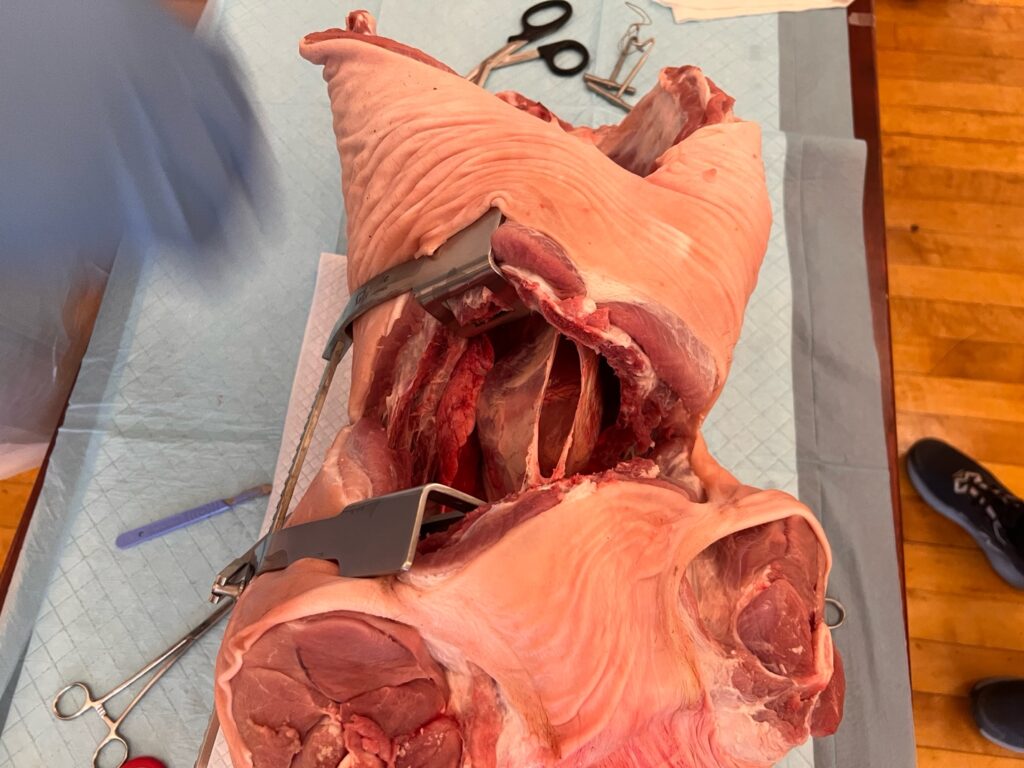
4. Clam-shell opening
- Cut the sternum with tough-cut scissors or a Gigli saw
- Insert Finochietto with handle toward axilla
- Spread ribs gradually
4. Manage the Lung
- Sweep left lung anteriorly/superiorly
- Control visible hemorrhage with pressure
5. Pericardiotomy
- Identify phrenic nerve
- Incise pericardium anterior to phrenic nerve
- Cephalad–caudal incision T-shaped incision with horizontal part of T towards base of the heart
- Evacuate blood and clot
If tamponade is present, decompression may immediately restore output.
6. Cardiac Assessment and Repair
- Deliver heart
- Identify injury
- Control bleeding with:
- Direct pressure
- Non-absorbable sutures
- Staples
- Foley catheter balloon tamponade (ventricular wounds)
- Avoid coronary vessel ligation.
7. Open Cardiac Massage
- One hand posterior, one anterior
- Compress apex to base
- ~80 compressions per minute
8. Aortic Occlusion
Indicated for:
- Exsanguinating infra-diaphragmatic hemorrhage
- Profound shock
Technique:
- Retract lung
- Identify descending aorta
- Manually occlude or apply cross-clamp
- Avoid clamping esophagus
- Clamp ideally just above diaphragm
Do not cross-clamp in normotensive patients.
9. Complications
Operator Risk
- Sharps injury from ribs or scalpel
- Blood-borne pathogen exposure
Procedural Complications
- Phrenic nerve injury
- Coronary artery injury
- Incomplete tamponade relief
- Aortic misidentification
- Distal organ ischemia from prolonged cross-clamp
Time and precision reduce harm.
10. Outcomes
Survival strongly correlates with:
- Mechanism (survival better in penetrating better than blunt)
- Cardiac injury location
- Presence of signs of life
- Time to intervention
Penetrating cardiac injuries with tamponade offer the best prognosis
Blunt trauma survival remains extremely low and controversial
11. HALO Teaching Framework
Recognition Drill
The candidate must verbalize:
- Mechanism
- Time since loss of vital signs
- Presence of signs of life
- Reversible pathology suspected
- Exit strategy (OT readiness)
Simulation Metrics
- Skin incision within 60–90 seconds of decision
- Correct intercostal space
- Pericardiotomy anterior to phrenic nerve
- Effective cardiac massage
- Correct aortic occlusion
Debrief Themes
- Was the indication correct?
- Was futility recognised appropriately?
- Was team communication clear?
- Was there an OR pathway?
12. Ethical Considerations
Resuscitative thoracotomy sits at the boundary of salvage and futility. HALO discipline demands:
- Decisive action in the salvageable
- Restraint in the unsalvageable
- Team consensus when possible
- Clear documentation of indications and time course
References:
- ATLS 10th Edition
- Tintinalli’s Emergency Medicine, 9th Edition
- Roberts & Hedges, 7th Edition
- Rosen’s Emergency Medicine, 10th Edition
- LITFL