1. Introduction
Pericardiocentesis is a high-risk, time-critical procedure performed to relieve pericardial pressure and restore cardiac output in cardiac tamponade. It may also be performed for diagnostic sampling of significant pericardial effusions.
In the HALO context, pericardiocentesis represents a rare but immediately life-saving intervention. Delay in tamponade leads rapidly to obstructive shock and cardiac arrest. However, inappropriate or poorly executed drainage may result in catastrophic complications including cardiac laceration, coronary injury, or death.
Modern practice strongly favors image-guided techniques, particularly echocardiography-guided drainage, which has dramatically reduced morbidity compared with historical blind approaches.
2. Learning Objectives
After completing this module, participants should be able to:
- Recognize clinical and sonographic signs of cardiac tamponade.
- Differentiate true tamponade from isolated echocardiographic chamber collapse.
- Identify optimal anatomical entry sites.
- Perform ultrasound-guided pericardiocentesis safely.
- Perform landmark subxiphoid drainage in resource-limited settings.
- Confirm guidewire position prior to dilation.
- Recognize and manage complications.
- Implement post-procedure monitoring and drainage strategy.
3. Anatomy and Physiologic Basis
Pericardial Anatomy
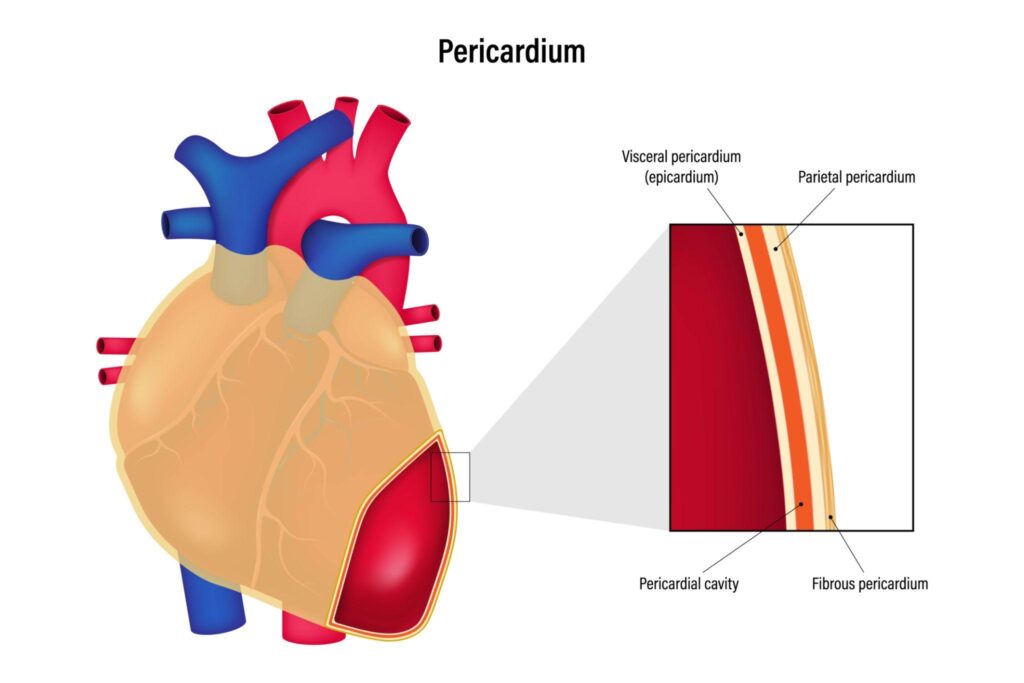
The pericardium consists of:
- Fibrous outer pericardium
- Serous pericardium (parietal and visceral layers)
- Normal fluid volume: 15–50 mL
Key relationships:
- Lungs (pleura laterally)
- Liver (subxiphoid approach)
- Coronary arteries
- Internal mammary vessels
- Phrenic nerve
Understanding these relationships is critical to avoid procedural injury.
Physiology of Tamponade
Cardiac tamponade occurs when intrapericardial pressure rises sufficiently to:
- Impair diastolic filling
- Reduce stroke volume
- Cause obstructive shock
Acute accumulation of 80–200 mL may cause collapse, whereas chronic effusions may exceed 1–2 L before decompensation.
Hemodynamic features:
- Hypotension
- Tachycardia
- Elevated JVP
- Pulsus paradoxus (>10 mmHg drop)
- Dyspnea
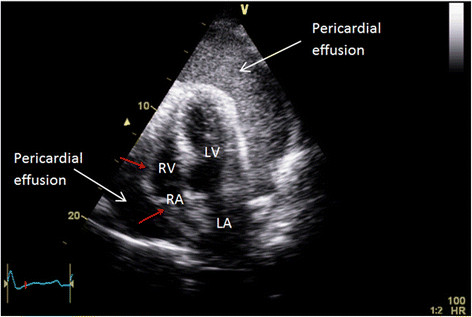
Echocardiographic signs alone do not equal tamponade. Clinical instability must be present.
4. Indications
Emergent (ED HALO Indication)
Cardiac tamponade with shock or peri-arrest
This is the primary emergency department indication.
Examples:
- Penetrating chest trauma with effusion
- Post-procedural iatrogenic perforation
- Malignant tamponade with shock
- Uremic effusion with instability
Urgent / Elective
- Large symptomatic effusion
- Suspected bacterial, TB, or neoplastic pericarditis
- Chronic large effusion >20 mm
Mild effusions without compromise should not undergo routine diagnostic drainage.
5. Contraindications
There are no absolute contraindications in unstable tamponade.
Relative contraindications:
- Aortic dissection (surgical tamponade)
- Post-MI free wall rupture
- Severe coagulopathy
- Anticoagulation
- Small loculated effusion
In selected unstable aortic dissection cases, small-volume controlled drainage may be used as a bridge to surgery.
6. Equipment
Essential equipment includes:
- Ultrasound (phased array preferred)
- 16–18G needle (long spinal or central line needle)
- 20 mL syringe with extension tubing
- J-tip guidewire
- 6–8 Fr dilator
- 6–8 Fr pigtail catheter
- 3-way stopcock
- ECG monitoring
- Sterile field and local anesthetic
HALO principle: use familiar central line equipment rather than unfamiliar specialty kits.
7. Technique
Preferred: Ultrasound-Guided (Real-Time)

4
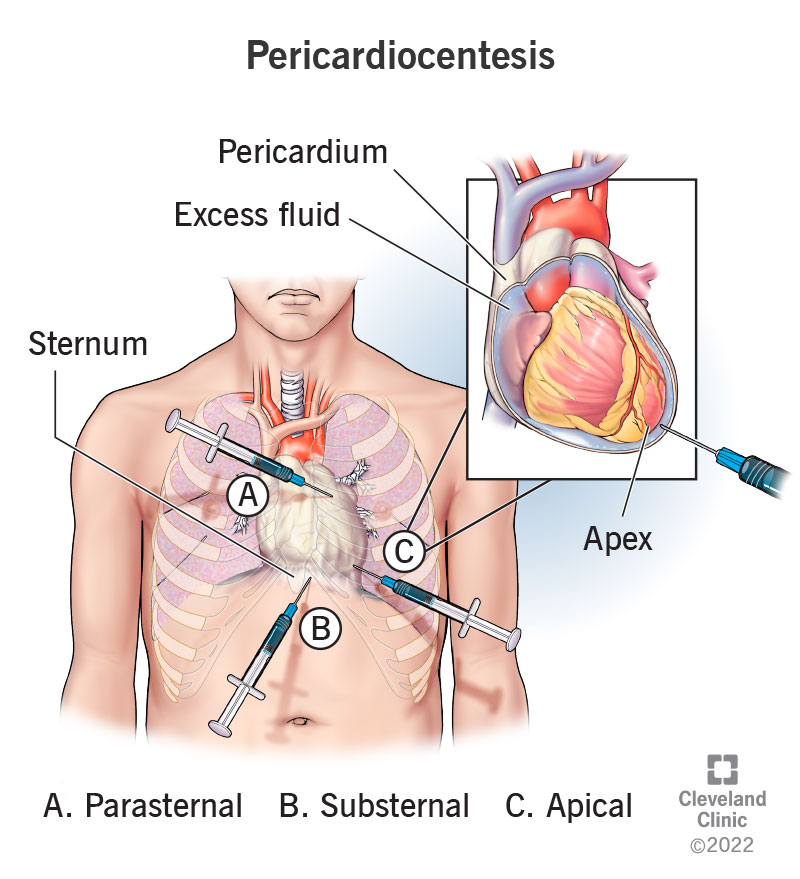
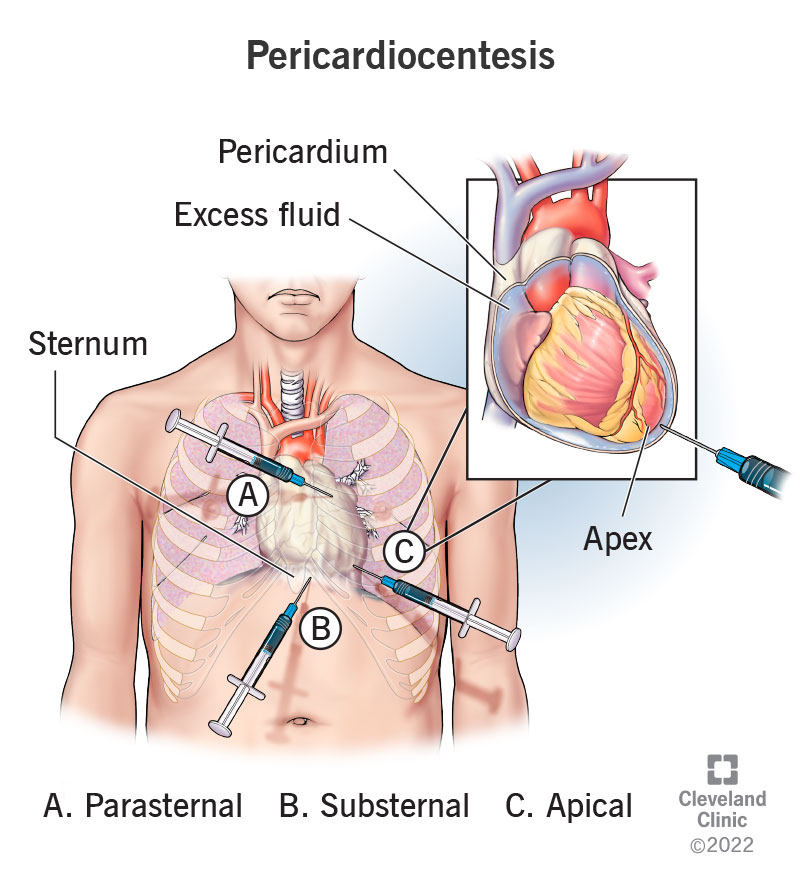
Step 1 – Identify Effusion
Use:
- Apical 4-chamber
- Parasternal long-axis
- Subxiphoid
Choose the shortest needle-to-fluid path without intervening lung or coronary vessels.
Step 2 – Patient Position
Semi-reclining at 30°, slight left rotation.
Step 3 – Needle Advancement
Advance under continuous visualization with aspiration.
Key principle: Always see the needle tip.
Step 4 – Confirm Pericardial Entry
- Fluid aspiration
- Agitated saline bubbles in pericardial space
- Hemodynamic improvement
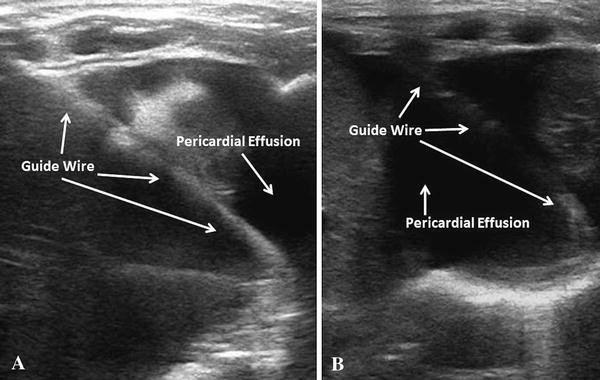
Step 5 – Guidewire Confirmation
Advance 20–30 cm or until resistance.
The wire should coil around the heart.
Confirm in multiple views before dilation.
Failure to confirm risks dilating into a cardiac chamber — life-threatening.
Step 6 – Seldinger Technique
- Dilate
- Insert pigtail catheter
- Attach to drainage system
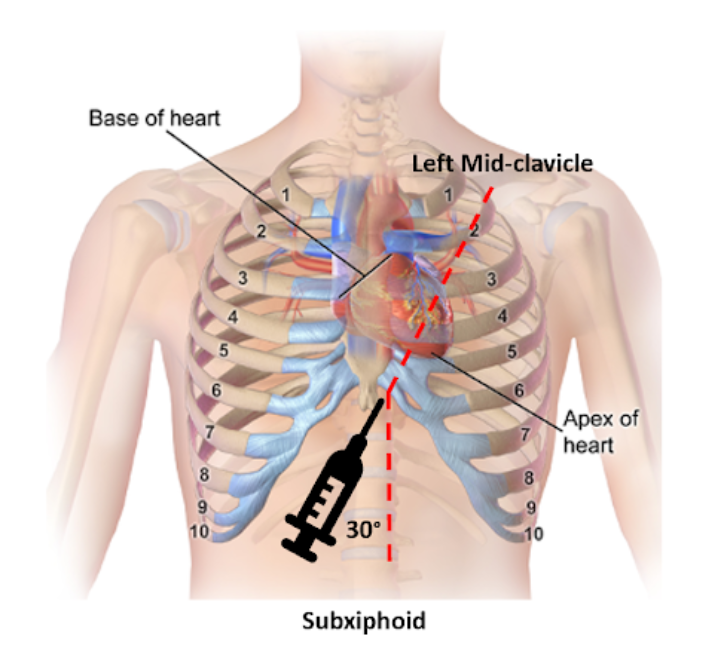
Landmark Subxiphoid Technique (Resource-Limited setting)
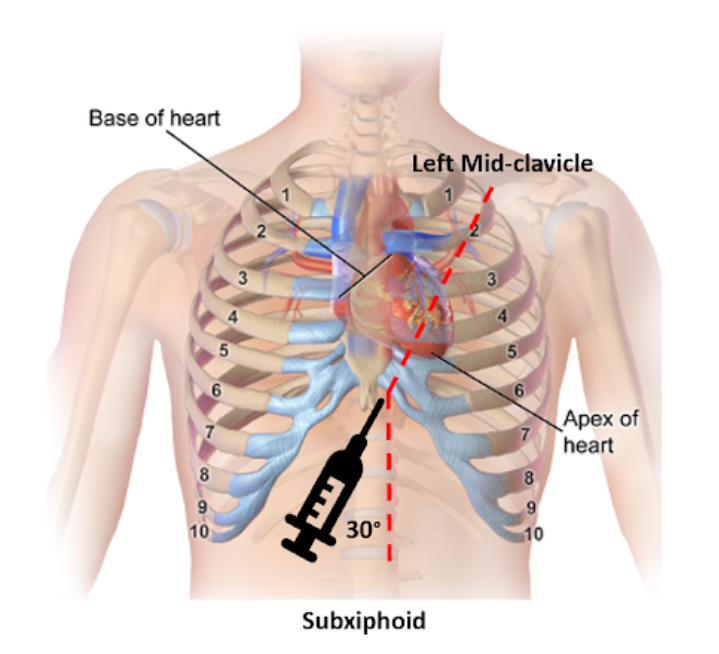
4
- Insert 1–2 cm below and left of xiphoid.
- Angle 15–30° toward left shoulder.
- Maintain continuous aspiration.
- ECG monitoring for ST elevation (myocardial contact).
This method carries higher complication risk and should be reserved for when imaging is unavailable.
8. Confirming Correct Placement
Methods include:
- Guidewire coiling on ultrasound
- Hemodynamic improvement
- Non-clotting blood
- Agitated saline bubble test
- Chest X-ray (post-procedure)
No single method is perfect.
9. Medical Temporization
If immediate drainage is delayed:
- 250–500 mL crystalloid bolus may transiently improve blood pressure.
- Avoid large volumes.
- Avoid diuretics.
- Positive-pressure ventilation may worsen tamponade.
This is a bridge — not definitive therapy.
10. Complications
Major complication rates are low when image guidance is used.
Serious complications:
- Myocardial laceration
- Coronary injury
- Internal mammary artery injury
- Pneumothorax
- Liver puncture
- Ventricular arrhythmias
- Pericardial decompression syndrome
- Death
Decompression syndrome may occur hours to days later; avoid draining very large volumes rapidly.
11. Post-Procedure Management
- Monitor in high-acuity setting
- Serial hemodynamic assessment
- Repeat ultrasound
- Drainage every 4–6 hours
- Remove catheter when <25–30 mL/24 hr
- Chest X-ray to exclude pneumothorax
Extended drainage reduces recurrence compared to single aspiration.
12. HALO Mindset Integration
Pericardiocentesis exemplifies HALO principles:
- Rare procedure
- Rapid deterioration if missed
- High consequence error profile
- Requires cognitive clarity under stress
Key safeguards:
- Use ultrasound whenever possible
- Confirm guidewire before dilation
- Stop if uncertain
- Maintain surgical backup
- Reassess continuously after decompression
13. Simulation Scenario
Scenario:
60-year-old with penetrating chest injury, PEA arrest. FAST positive for pericardial fluid.
Objectives:
- Recognize tamponade
- Perform ultrasound-guided drainage
- Confirm guidewire placement
- Achieve ROSC
Assessment:
- Needle visualization
- Fluid aspiration
- Hemodynamic improvement
- Safe catheter placement
14. Clinical Significance
Pericardiocentesis is a life-saving maneuver in obstructive shock. Prognosis post-procedure depends on etiology:
- Excellent in viral/idiopathic cases
- Guarded in malignant disease
Mastery requires structured training, repetition, and disciplined technique. In the HALO environment, competence must be present before the rare moment demands it.