Dr Parul Chandra, Mr SP Singh
High Acuity, Low Occurrence (HALO) Emergency Airway
1. Introduction
Surgical cricothyrotomy is the definitive rescue airway in a cannot intubate, cannot oxygenate (CICO) scenario. When conventional airway techniques fail and hypoxia is imminent, establishing front-of-neck access is lifesaving.
Cricothyrotomy is preferred over emergency tracheostomy in adults because it is faster, requires less equipment, and is technically simpler
Cricothyroidotomy
In HALO terms, surgical cricothyrotomy is:
- High Acuity – failure results in hypoxic arrest
- Low Occurrence – rarely performed in modern practice
- Time Critical – decision-to-incision delay kills
- Skill Dependent – anatomy and tactile control are essential
2. Learning Objectives
After completing this module, participants should be able to:
- Recognize CICO and commit to front-of-neck access early.
- Identify cricothyroid membrane (CTM) anatomy reliably.
- Perform the scalpel–bougie–tube technique.
- Demonstrate procedural competence within simulation time standards.
3. Anatomy and Clinical Context
The cricothyroid membrane lies:
- Superiorly: Thyroid cartilage
- Inferiorly: Cricoid cartilage
- Laterally: Cricothyroid muscles
It is located approximately 2 cm below the laryngeal prominence
The CTM is the most accessible site for emergency airway entry. Several vascular structures are nearby, including branches of the superior thyroid artery and anterior jugular veins
Practical Reality
In thin patients, landmarks are clear.
In obese, bleeding, or trauma patients, they are not.
This is a tactile procedure. Vision will be limited by blood. You must rely on palpation
Make a vertical midline incision and identify structures with your finger
4. Indications
Emergency cricothyrotomy is indicated in any CICO scenario. It is the final step in the difficult airway algorithm. Delay leads rapidly to hypoxia, brain injury, and death.
5. Contraindications
There are no absolute contraindications
6. Equipment
Essential tools:
Source: DAS Guidelines UK 2025
- #10 scalpel
- Bougie
- 6.0 cuffed endotracheal tube
- 10 mL syringe
- Suction
- Oxygen source
A 6.0 ETT approximates the diameter of the adult CTM (~1 cm)
7. Preparation
In CICO:
- Do not delay for consent
- Do not delay for imaging
- Do not delay for sterility perfection
If possible:
- Apply antiseptic
- Wear PPE
- Ensure suction available
Cognitive aids and hard stops in airway algorithms improve timely decision-making
8. Technique — Scalpel–Bougie–Tube
The preferred method in emergency medicine is the stab-twist-bougie-tube technique
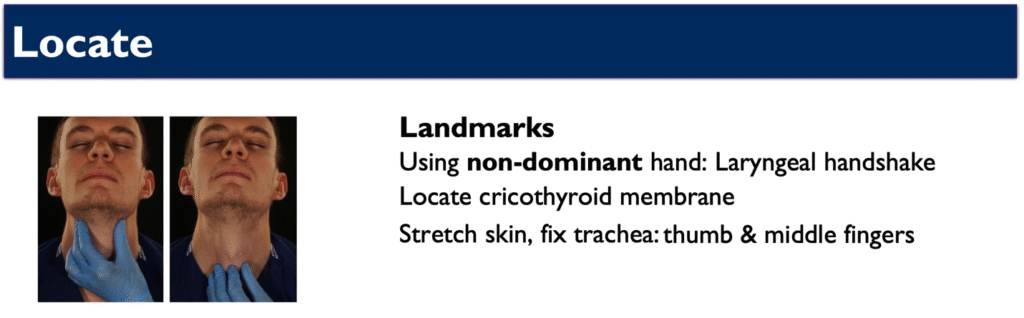
Step 1 – Laryngeal Handshake
Source: DAS Guidelines UK 2025
- Right-handed operator stands on left side of the patient
- Grasp thyroid cartilage between thumb and middle finger
- Stretch skin taut
- Palpate CTM with index finger
This stabilizes the larynx and defines midline.
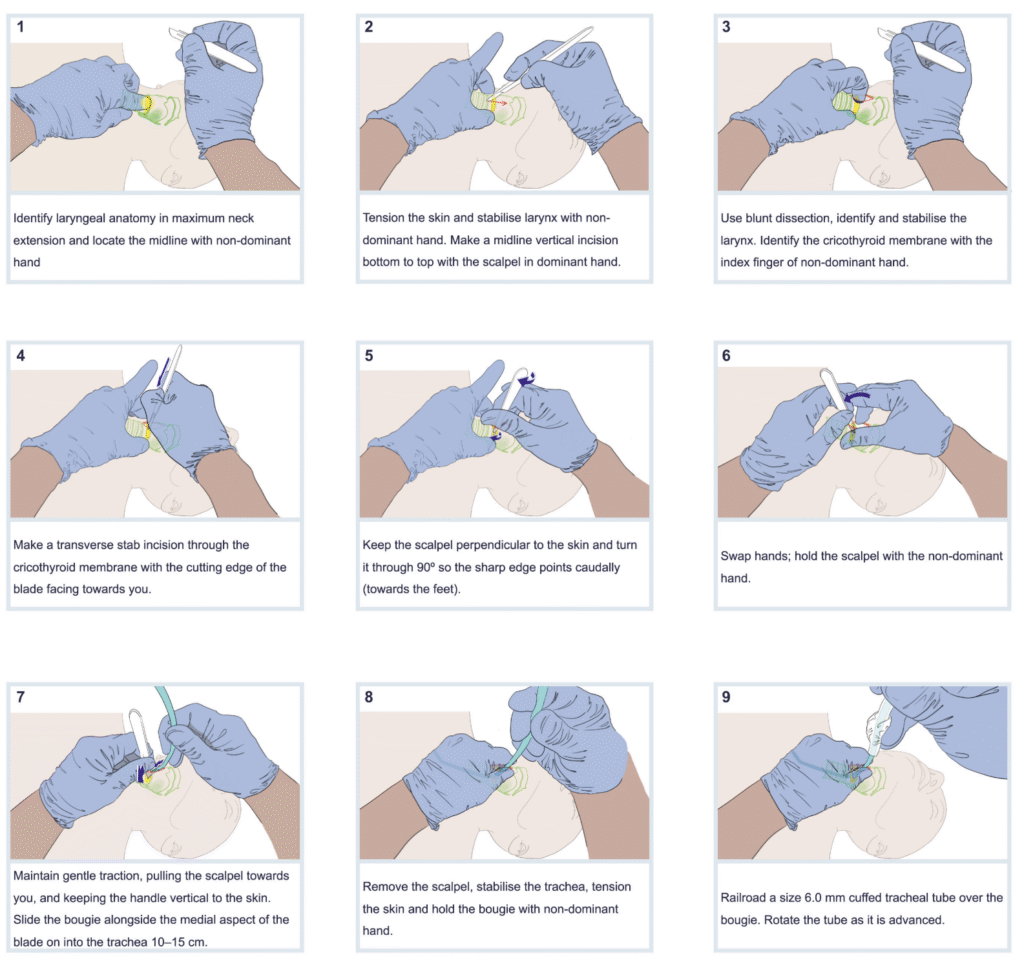
Step 2 – Stab
- Hold scalpel in dominant hand
- Midline vertical incision up to 8 cm
- Use blunt dissection with fingers of both hands to separate tissues
- Use the nondominant hand index finger to identify CTM
- With scalpel in dominant hand Transverse stab incision, cutting edge towards you
Step 3 – Twist
- Keep scalpel perpendicular to patient
- Twist scalpel through 90 degrees, cutting edge caudad
- Traction on scalpel towards you, handle upright, swap hands: hold scalpel with nondominant hand
- Take bougie in dominant hand
Step 4 – Bougie Insertion
- Slide bougie down into trachea, by the side of scalpel
- Rotate and align the bougie with the trachea and advance gently to 10-15 cm
- Remove the scalpel
Go in with 90-degree angle of the tip of bougie with tracheal hole — prevents false tract.
Step 5 – Tube Placement
- Railroad 6.0 cuffed ETT over bougie
- Rotate the tube as it is advanced until cuff passes CTM
- Remove bougie
- Inflate cuff
- Ventilate with 100% oxygen
Source: DAS Guidelines UK 2025
Step 6 – Confirmation
Confirm placement by waveform capnography
Secure tube immediately.
9. Monitoring
After placement:
- Continuous capnography
- Pulse oximetry
- Blood pressure monitoring
- ECG if available
10. Complications
Early
- Bleeding (common)
- False tract formation
- Posterior tracheal injury
- Endobronchial intubation
- Hypoxia from delay
Bleeding should be managed with direct pressure. Tactile guidance may be required
Late
- Subglottic stenosis
- Dysphonia
- Fistula formation
Reported complication rates vary widely (0–54%) depending on setting and expertise
In CICO, benefits outweigh risks.
11. Common Technical Errors
- Hesitation after CICO recognition
- Incision too small
- Incision off midline
- Bougie inserted into soft tissue
- Tube advanced too far (right mainstem)
The most lethal error is delay.
12. Simulation Performance Criteria
Participants must:
- Recognise CICO promptly
- Perform vertical and horizontal incisions correctly
- Insert bougie accurately
- Confirm placement with ETCO₂
Regular multidisciplinary rehearsal improves outcomes
13. Summary
Surgical cricothyrotomy is the final, decisive step in airway rescue. It is a simple, reproducible technique that requires:
- Early recognition
- Anatomical confidence
- Decisive action
In HALO practice, competence in cricothyrotomy prevents preventable hypoxic death.
References
- Ahmad, Imran et al. British Journal of Anaesthesia, Volume 136, Issue 1, 283 – 307 Difficult Airway Society 2025 guidelines for management of unanticipated difficult tracheal intubation in adults
- Frerk C, Frampton C. Cricothyroidotomy; time for change. Anaesthesia. 2006 Oct;61(10):921-3. PMID: 16978303.
- Hessert MJ, Bennett BL. Optimizing emergent surgical cricothyrotomy for use in austere environments. Wilderness Environ Med. 2013 Mar;24(1):53-66. doi: 10.1016/j.wem.2012.07.003. Epub 2012 Oct 10. PMID: 23062323.
- Hill C, Reardon R, Joing S, Falvey D, Miner J. Cricothyrotomy technique using gum elastic bougie is faster than standard technique: a study of emergency medicine residents and medical students in an animal lab. Acad Emerg Med. 2010 Jun;17(6):666-9. PMID: 20491685
- Langvad S, Hyldmo PK, Nakstad AR, Vist GE, Sandberg M. Emergency cricothyrotomy–a systematic review. Scand J Trauma Resusc Emerg Med. 2013;21:43
- Mabry RL, Nichols MC, Shiner DC, Bolleter S, Frankfurt A. A comparison of two open surgical cricothyroidotomy techniques by military medics using a cadaver model. Ann Emerg Med. 2014 Jan;63(1):1-5. PMID: 24094476.
- Paix BR, Griggs WM. Emergency surgical cricothyroidotomy: 24 successful cases leading to a simple ‘scalpel-finger-tube’ method. Emerg Med Australas. 2012 Feb;24(1):23-30. PMID: 22313556.
- Wong DT, Prabhu AJ, Coloma M, Imasogie N, Chung FF. What is the minimum training required for successful cricothyroidotomy? a study in mannequins. Anesthesiology. 2003 Feb;98(2):349-53. PMID: 12552192.